The term biofeedback has come to be defined as the process of monitoring some biological event with an instrument designed to provide real-time information about that event to the person being monitored. However, clinical biofeedback requires accurate measurement of various physiological processes while providing the client feedback that is sensitive to small changes in his or her physiology. It is also necessary to provide instructions to the client about proper interpretation of the feedback signal and to emphasize why changing the physiology will treat the disorder. Generalization, the ability to transfer what is learned in the clinic to the person’s, home, work, and social environments, is also necessary.
Most biofeedback systems are computer interfaced so the feedback signal can be visual and/or auditory. The visual feedback is only limited by the computer graphics, so the signal can be as simple as a line graph where the status of the physiology is depicted by a line that moves across the screen, with the height of the line carrying the information about the level of the physiological event. In some instances, the feedback may be entertaining. This type of feedback is often used with children and can be, for example, a video game where the game’s progress is based on the level of the physiological event. For instance, a maze is presented that must be negotiated, with an object that moves through the maze one step each time the physiological event reaches a predetermined level. In these instances, the feedback is not only informative, but provides an incentive to the client to change his or her physiology in order to “play” such a game.
The physiological parameters used in clinical settings are levels of skeletal muscle activity (tested with electromyograms, EMG), finger skin temperature, sweat gland activity (measured as skin conductance activity, SCA), heart rate, brain wave activity (measured with quantitative electroencephalography, QEEG), and respiration events. Biofeedback of muscle activity is used to reduce sustained muscle activity, which often causes pain; to increase muscle activity after paralysis; and to re-educate specific muscle control after injury to the nervous system such as a stroke. Finger temperature biofeedback is often provided as an indicator of general relaxation because most individuals increase their finger temperature as they go from a stress response to being relaxed. Sweat gland activity is used as a measure of general arousal, especially to emotionally laden cognitive events. Heart rate is also often used as an indication of relaxation because when a person relaxes, the heart rate slows and produces certain rhythms. Brain wave biofeedback is used to treat such disorders as Attention Deficit/Hyperactivity Disorder (ADHD). When brain wave feedback is used it is usually based on findings that indicate the person has a specific brain wave that is related to his or her disorder and the biofeedback system is capable of detecting this activity and letting the person know when it is present. This information allows the person the possibility to either increase or decrease that activity, and thus have less of an unwanted activity and/or more of a wanted activity. Respiration biofeedback is often used as a means to teach correct breathing patterns and as a form of relaxation training.
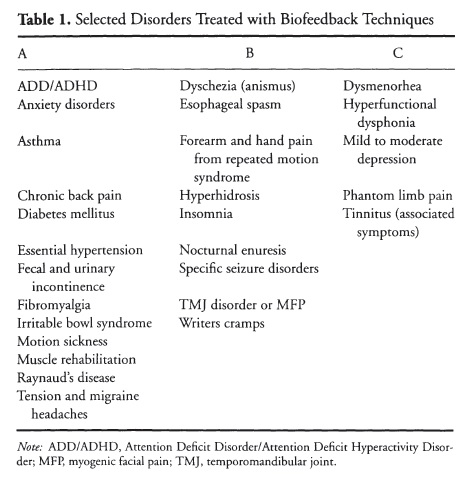
To present the disorders treated with biofeedback techniques, a table of these disorders was developed (see Table 1). Any listing of disorders should be taken as a guideline as it is always biased by the interpretation and experiences of the author. Some applications appear well established by controlled outcome studies of clinical effectiveness and cost effectiveness, whereas others are based on repeated single-case studies or multiple studies with relatively small sample sizes. Additionally, some applications are based on the clinical literature and the clinical experience of the author. The listing of disorders treated with biofeedback is divided into three categories: A = well established; B = multiple research support; but not enough to firmly substantiate the application; and C = promising but not established at this time.
The following are important when considering the application of clinical biofeedback for an individual: the individual must be able to tolerate the application of the sensors; be able to understand the instructions regarding the relationship between his or her physiology and the feedback signal; be motivated to change physiology, using the feedback signal to facilitate this process; and, finally, be motivated to practice what has been learned in the clinic in the world outside the clinic. One of the most frequent applications of biofeedback is to use it to facilitate relaxation training. This is referred to as biofeedback-facilitated relaxation training (BFRT).
Example of BFRT Protocol
When using BFRT, it is first necessary to determine whether the client would benefit from such therapy. General relaxation may be helpful in a variety of conditions and it may also be useful as an incompatible response during such procedures as systematic desensitization. BFRT normally takes between 8 and 20 sessions, depending on the acquisition skills and the distress level of the client before and during therapy. After determination of the need for BFRT, the therapist must explain the rationale for biofeedback therapy, outline the basic aspects of the physiological processes that will be trained, and discuss the potential benefits and risks of the training. This author recommends conducting the first BFRT session with frontal EMG feedback while monitoring other modalities such as finger temperature, SCA, and/or heart rate. During the first biofeedback session, facial muscle discrimination training should be demonstrated and the client should be provided time to use his or her relaxation techniques to reduce frontal EMG levels. The therapist should monitor the other modalities during the session to observe the changes that occur as the client tries to reduce frontal EMG levels. The value of monitoring other modalities is that, for instance, by observing sweat gland activity, it can be determined whether the client is engaging in arousing internal dialogue by noting whether several short duration responses are observed. If so, the therapist could interrupt the session and suggest a change in strategy by the client. During the interruption, the therapist should ask the client what strategy he or she was using and then encourage him or her to select a different strategy, such as diaphragmatic breathing or changes in imagery. The most labile physiological process is usually selected as the target of biofeedback therapy after frontal EMG levels are acceptable.
Another example of an often-used biofeedback procedure is QEEG feedback for treatment of ADHD: First, it is helpful to explain that the QEEG is different than the traditional EEG. The QEEG is the EEG after it has been digitized through the use of an analogue-to-digital converter. This process allows the mathematical determination of the characteristics of specific frequencies. Children with ADHD have been shown to have different patterns of brain waves then non-ADHD children of the same age. The diagnosed children have more electrical activity in the slow frequency range, such as theta (4-8 Hz) and alpha (8—12 Hz), and fewer in the fast frequency range, such as sensorimotor rhythm (SMR; 12-15 Hz) and beta (16-30 Hz). The biofeedback technique trains for a decrease in theta or alpha and an increase in SMR or beta. The treatment protocol requires a QEEG assessment to determine which specific frequencies will need to be trained. Several studies clearly demonstrate that the QEEG patterns change according to the direction of training for some children and that clinical improvements are observed with successful training. The number of sessions necessary is usually 40-60, depending on how quickly the QEEG changes. See Lubar (2003) and Lubar and Lubar (1999) for further information.
Summary
To be effective in the clinical application of biofeedback, one must have the following: a measurable physiological process, feedback about the process provided with enough resolution and speed to allow the individual to obtain volitional control of the physiology, and a change in physiology that alters the physiological processes causing the targeted disorder. In some instances the relationship between the monitored physiological event and the disorder is obvious, such as finger temperature for Raynaud’s disease, but for others, such as BFRT for the treatment of asthma and irritable bowel syndrome, the relationship is less obvious. Therefore, the clinician must be aware of the physiology underlying the disorder and the literature that relates to the different biofeedback treatments used to treat it. This information must then be combined with the individual’s characteristics such as his or her unique physiological levels and the ability to benefit from the various types of biofeedback techniques available. The clinician must also be skilled in helping the client transfer the control acquired in the clinic to the individual’s life situations. Constant advances in computer technology and developments in bioengineering, which provide new sensor technology and signal processing, make the future of clinical biofeedback look very promising.
References:
- Evans, J. R., & Abarbanel, A. (Eds.). (1999). Introduction to quantitative EEG and biofeedback. New York: Academic.
- Lubar, J. F. (2003). Neurofeedback for the management of attention-deficit/hyperactivity disorders. In M. S. Schwartz (Ed.), Biofeedback: A practitioner’s guide (3rd ed.). (pp. 493-522). New York: Guilford.
- Lubar, J. E, & Lubar, J. O. (2003). Neurofeedback assessment and treatment for attention deficit/hyperactivity disorders. In J. R. Evans & A. Abarbanel (Eds.), Introduction to quantitative EEG and neurofeedback (pp. 103-143). San Diego: Academic.
- Kasman, G. S., Cram, J. R., Wolf, S. L., & Barton, L. (1998). Clinical applications in surface electromyography: Chronic musculosketal pain. Gaithersberg, MD: Aspen.
- Schwartz, M., &: Andrasik, F. (Eds.). (2003). Biofeedback: A practitioners guide. New York: Guilford.
Back to Health Psychology.