Physical activity is bodily movement produced by the contraction of skeletal muscle that increases energy expenditure above the basal level. In contrast, exercise denotes a subcategory of physical activity that is planned, structured, repetitive, and purposive in the sense that improvement or maintenance of one or more components of physical fitness is the objective. Physical fitness, generally considered a product of both genetics and physical activity, is the ability to carry out daily tasks with vigor and alertness, without undue fatigue, and with ample energy to enjoy leisure-time pursuits and to meet unforeseen emergencies. The most commonly used measure of physical fitness is the ability of the circulatory and respiratory systems to supply oxygen during sustained physical activity, and is referred to as cardiorespiratory or cardiovascular fitness. Physical activity, then, is the more general category that encompasses exercise and largely determines physical fitness.
Physical Activity and Physical Health
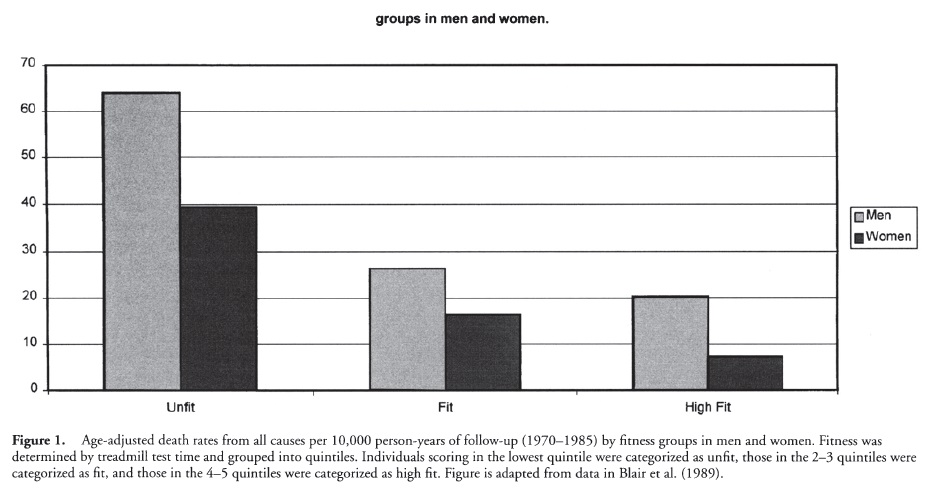
Physical fitness and physical activity are undeniably beneficial for physical health. Both men and women with higher levels of cardiovascular fitness have a decreased risk of dying from all causes (see Figure 1), from cardiovascular disease, and from cancer, and a similar relationship has been found between physical activity and mortality from all causes, cardiovascular disease, and cancer.
Physical activity also has positive effects on several chronic health conditions, namely, obesity, Type 2 diabetes, and osteoporosis. As the most variable component of energy expenditure, physical activity can influence the development of obesity as well as success in achieving both initial and long-term weight loss. Physical activity also reduces the likelihood that a person at risk for Type 2 (adult-onset) diabetes will develop the disorder and enhances blood glucose regulation in those with the disease. With respect to osteoporosis, the National Institutes of Health recommends that physical activity should be encouraged during childhood and adolescence to promote optimal bone growth and reduce the risk of osteoporosis later in life, whereas those with osteoporosis should engage in physical activity both to slow down bone loss and to lower the risk of falls.
Physical Activity and Psychological Well-Being
Many people believe that physical activity improves psychological well-being, and a large number of studies have sought to demonstrate that physical activity elevates mood, reduces depression, and alleviates anxiety. A review of the evidence reveals a strong consensus among researchers that mood enhancement is a primary benefit of physical activity. Similarly, physical activity has been useful in ameliorating mild to moderate depression. Some studies also have shown that physical activity reduces anxiety, defined as a feeling of apprehension or fear that lingers, though the evidence for this link is less consistent.
How Much Physical Activity is Enough?
Knowing that more active individuals are healthier than less active individuals brings up two related questions:
- How much physical activity is enough?
- What type of physical activity is most effective?
In terms of the benefits of physical activity for physical health, the single most important factor may be total energy expenditure. Among sedentary, unfit adults, the accumulation of 30 min of walking per day (or the equivalent energy expenditure in other activities) is likely to result in clinically significant health benefits. This approach to physical activity, in which the emphasis is on accumulation of moderate-level activity, has been described in terms of promoting lifestyle activity. Some evidence suggests that among adults lifestyle activity may bring about positive health effects comparable to those of a programmed exercise regimen, and that individuals may be more likely to maintain the former than the latter.
These recommendations have been generated in reaction to the public health issue posed by the great number of adults in the United States who engage in little or no activity beyond that required for daily living. Thus, an emphasis has been placed on motivating these sedentary persons to engage in at least a minimal level of activity that would bring about meaningful health improvements. Moreover, the greatest differential in health outcomes is between adults who engage in virtually no activity and those who engage in activity equal to at least 30 min of brisk walking per day (see Figure 1). Combined with evidence that improvements in cardiovascular fitness may be achieved through accumulated short, intermittent bouts of activity, the result has been a shift away from earlier recommendations that emphasized continuous bouts (i.e., 30 min or more) of relatively vigorous activity. It is likely, however, that the frequency, duration, intensity, and type of activity that will promote optimal health will vary from person to person and across different health outcomes. For example, the amount and type of activity that promotes optimal bone health may differ from the amount and type of activity that promotes optimal psychological well-being.
An additional level of complexity is introduced when focusing on the psychological benefits of physical activity. Although some psychological benefits of physical activity may be related to underlying changes in physiology that occur in response to exercise, it is generally believed that benefits also may derive from nonphysiological aspects of physical activity, such as social interaction, distraction, or simple enjoyment of the activity. Moreover, the likelihood that an individual will adhere to an activity prescription must be considered. Because adherence is critical to achieving health benefits, the choice of activity thus becomes an essential consideration in any exercise prescription.
Common Strategies to Promote Physical Activity
A number of strategies have been employed to promote physical activity in individuals and/or communities. Approaches that have shown evidence of being effective include the following:
- Point-of-decision prompts are signs placed by elevators and escalators to motivate people to use nearby stairs.
- Community-wide campaigns typically involve many sectors of the community, combine multiple intervention approaches, and employ a highly visible communication campaign linking all elements into an integrated program.
- School-based physical education involves modifying school curricula and policies to increase the amount of time that students spend in moderate or vigorous activity while in physical education classes.
- Social support interventions in community settings focus on changing physical activity behavior by encouraging supportive relationships for behavior change; for example, programs may set up a “buddy” system or set up walking groups.
- Individually adapted health behavior change programs are tailored to the individual, and teach participants behavioral skills that enable them to incorporate physical activity into daily routines.
Exercise Promotion in Special Populations
Because physical activity has important health benefits in youth and many young people are not meeting established guidelines, improving the physical activity levels of youth is an important public health challenge. Recommended levels of activity for youth range from 30 to 60 min per day of moderate-to-vigorous activity. Unfortunately, social and economic forces have restricted opportunities for children and adolescents to be physically active while trends in leisure-time activities have increased time spent in sedentary activities such as watching television and playing video games. In reaction to these trends, programs have been designed to enhance access to facilities for activity, bolster participation in school-based physical education, and reduce television watching.
The elderly also stand to benefit considerably from increased physical activity both in terms of quality of life and health outcomes. Physical activity typically declines with age, and age-associated illness further contributes to a decline in activity among the elderly. In addition to the demonstrated benefit of physical activity for reducing all-cause mortality, participation in physical activity has shown promise among the elderly for ameliorating several age-associated declines in function, including cognitive function, cardiovascular fitness, and muscle and bone strength. Importantly, exercise that is initiated in late life, even after a sedentary middle age, may result in substantial gains in life expectancy.
In sum, physical activity is consistently and strongly related to multiple dimensions of health and offers an effective means of reducing morbidity and mortality. Physical activity is valuable in the prevention and treatment of obesity, diabetes, osteoporosis, depression, and heart disease. Because of the large proportion of the U.S. population that is sedentary, the promotion of physical activity has huge potential for enhancing public health. Moreover, meaningful health benefits may be realized by accumulating as little as 30 min per day of moderate activity, though more and/or more intense activity may be required to bring about specific improvements such as enhanced cardiovascular fitness or weight loss. The benefits are particularly evident among youth and the elderly, both of whom stand to gain enormously from adopting and maintaining an active lifestyle.
References:
- Berger, B., & Mod, R. (2000). Exercise and mood: A selective review and synthesis of research employing the Profile of Mood States. Journal of Applied Sport Psychology, 12, 69-92.
- Blair, S., Cheng, Y., & Holder, J. S. (2001). Is physical activity or physical fitness more importnat in defining health benefits? Medicine and Science in Sports and Exercise, 33(6 Supplement) S379-S399.
- Blair, S., Kohl, H., Gordon, N., & Paffenbarger, Jr., R. (1992). How much physical activity is good for health? Annual Review of Public Health, 13, 99-126.
- Blair, S., Kohl, H., Paffenbarger, R., Clark, D., & Cooper, K. (1989). Physical fitness and all-cause mortality; A prospective study of healthy men and women. Journal of the American Medical Association, 262, 23952401.
- DeBusk, R., Stenestrand, U., Sheehan, M., & Haskell, W. (1990). Training effects of long versus short bouts of exercise in healthy subjects. American Journal of Cardiology, 65, 1010-13.
- Dunn, A., Trivedi, M., & O’Neal, H. (2001). Physical activity dose-response effects on outcomes of depression and anxiety. Medicine and Science in Sports and Exercise, 33(6 Supplement), S587-S597.
- Kahn, E. B., Ramsey, L. T, et al. (2002). The effectiveness of interventions to increase physical activity: A systematic review. American Journal of Preventive Medicine, 2(48), 73-107.
- Kelley, D., & Goodpaster, B. (2001). Effects of exercise on glucose homeostasis in Type 2 diabetes mellitus. Medicine and Science in Sports and Exercise, 33(6 Supplement), S495-S501.
- King, A., & Tribble, D. (1991). The role of exercise in weight regulation in nonathletes. Sports Medicine, 11, 331-349.
- National Institutes of Health. (2000). Osteoporosis prevention, diagnosis, and therapy [NIH Consensus Statement 17(1)]. Bethesda, MD: Author.
- Sallis, J. E, Prochaska, J. J., & Taylor, W. C. (2000). A review of correlates of physical activity of children and adolescents. Medicine and Science in Sports and Exercise, 32, 963-975.
- U.S. Department of Health and Human Services. (1996). Physical activity and health: A report of the surgeon General. Atlanta, GA: Centers for Disease Control and Prevention.
- Wagner, E. H., LaCroix, A. Z., Buchner, D. M., & Larson, E. B. (1992). Effects of physical activity on health status in older adults I: Observational studies. Annual Review of Public Health, 13, 451-468.
Back to Health Psychology.