Self-regulation refers to the processes by which individuals control or direct their thoughts, emotions, and actions to achieve their goals. According to self-regulation theory, behavior is guided by a motivational system of setting goals, developing and enacting strategies to achieve those goals, evaluating progress, and revising goals and actions accordingly. Increasingly, self-regulation models are being used to explain health behaviors taken to achieve goals of improving health, such as through changes in exercise or diet behaviors, and goals of avoiding illnesses and their consequences, such as through seeking medical care for unusual symptoms or adhering to medical treatments.
Fundamental to self-regulation models is the concept of feedback. When individuals perform behaviors, they search for and appraise information about the outcomes of the behaviors in terms of their success in moving them toward their desired states. This feedback process helps individuals keep on track in their efforts to attain their goals. Another aspect of self-regulation models is an emphasis on the role of emotions in motivating and guiding behavior. These models focus on how fear, joy, and other emotions influence the selection of goals and behaviors.
The concepts of self-control and will power are also important. Many health behaviors such as regular exercise, smoking cessation, and medication adherence require individuals to refrain from indulging in gratifying substances and activities or, alternatively, to engage in uncomfortable or inconvenient activities. According to self-regulation models, it is necessary to pay consistent attention to behavior and goals to maintain the self-control and will power needed to sustain these behaviors over time. Self-monitoring techniques, which involve recording behaviors in a log or diary, can help individuals keep their attention focused on the behaviors and their progress. For example, use of a daily log of food intake can improve individuals’ success in losing weight.
Two models frequently used in health psychology research are Charles Carver’s and Michael Scheier’s self-regulation model and Howard Leventhal’s commonsense model. The former is a model of general behavior that has been used to guide research on health and illness behaviors and outcomes, whereas the latter model focuses specifically on illness-related behaviors.
Carver and Scheier’s Model of Self-Regulation
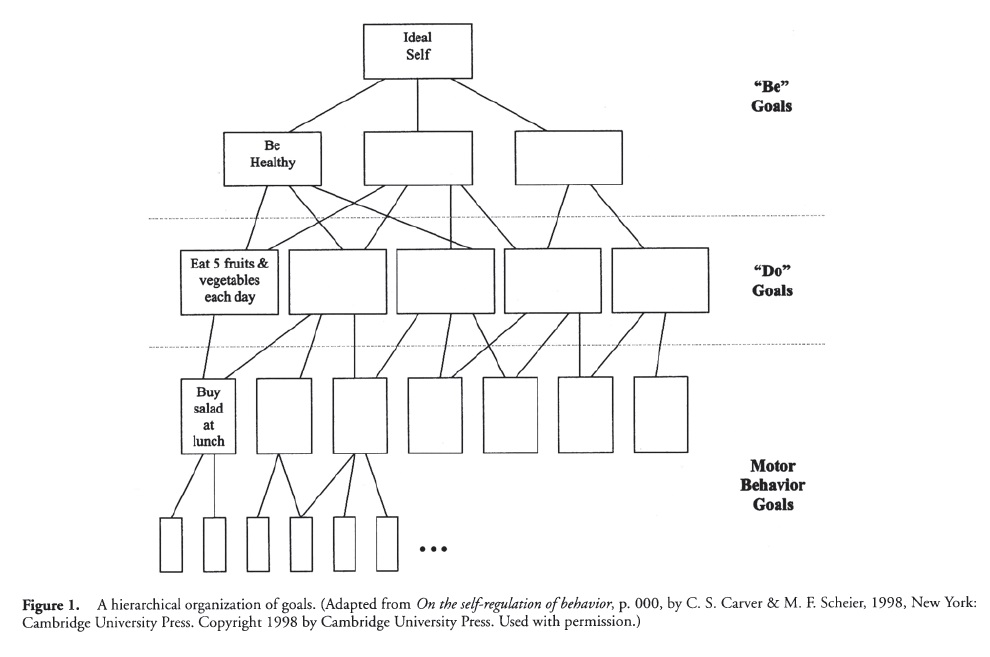
Carver and Scheier’s model of self-regulation focuses on how people go through their daily activities by selecting goals and then choosing behaviors accordingly. According to this model, health behaviors can best be understood by considering how they relate to the individual’s life goals. An individual can have many related goals (see Figure 1); for example, an individual can have a relatively abstract goal to “stay healthy,” a more specific goal to “eat five fruits or vegetables each day,” and an even more specific goal to “buy a salad at lunchtime.” These goals have a hierarchical organization, with goals about the type of person one would like to “be” on top. These goals link with goals involving the kinds of actions one needs to “do,” which in turn connect with more specific goals concerning motor behavior sequences involved in the action. Goals can also vary in terms of whether they involve approach or avoidance behaviors, that is, whether they involve moving a person toward a desired state (e.g., physical fitness) or away from an undesired state (e.g., getting HIV/AIDS).
The model also identifies how different emotional experiences occur during efforts to achieve goals. Wflien individuals believe they are making good progress toward a desired goal (approach behavior), then they will experience positive affect such as pleasure or happiness. When they believe they are not making progress toward desired states, then negative affect such as depression will arise. Different kinds of positive and negative emotions are associated with avoidance goals and behaviors. When individuals believe they are doing well in avoiding undesirable states, they experience relief; when they feel their avoidance attempts are unsuccessful, they experience anxiety.
Expectancies as Determinants of Behavior
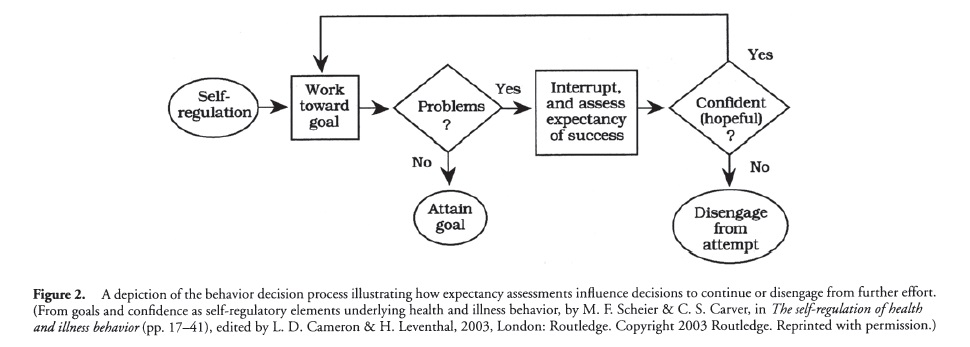
According to the Carver and Scheier model, expectancies play a critical role in self-regulation. Individuals typically encounter problems and challenges as they work toward their goals. Whether they continue to pursue those goals depends on their expectancies about their potential success (see Figure 2). If they feel confident that they can achieve their goals, they continue their efforts. If they have doubts, they are likely to give up. When beginning an exercise program, for example, efforts to maintain the program will depend on whether one has confidence that the exercise goal can be achieved.
Research has shown that individuals vary in their generalized expectancies, that is, their tendencies to expect positive or negative outcomes when facing uncertain conditions. Dispositional optimism is a personality characteristic involving the tendency to expect positive outcomes and to feel confident that one’s goals will be attained. Compared to individuals who are low in dispositional optimism, those high in dispositional optimism tend to experience more positive emotions and show more persistence in goal-related efforts. These tendencies appear to have beneficial health effects. In studies conducted by Scheier and colleagues in 1989 and 1999 of individuals undergoing coronary artery bypass surgery, patients with high (versus low) dispositional optimism had faster recovery rates and a reduced likelihood of being rehospitalized in the months following surgery.
Leventhal’s Commonsense Model of Self-Regulation
The commonsense model focuses on cognitions, emotions, and actions elicited in response to health threats. It gives particular emphasis to individuals’ personal beliefs about illnesses and their commonsense rules for making health-related decisions. According to this model (see Figure 3), the perception of health threat cues simultaneously activates problem-focused self-regulation (efforts to control the health threat itself) and emotion-focused self-regulation (efforts to manage emotional distress).
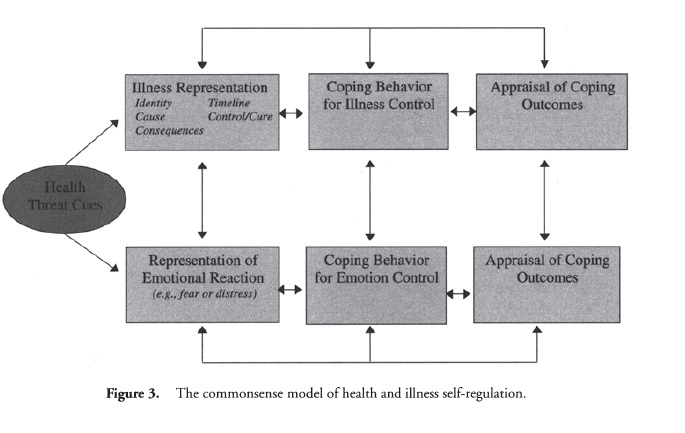
At the problem-focused level, threatening cues (e.g., symptoms such as wheezing and difficulty breathing) elicit the activation and development of a cognitive representation of the health threat. This representation includes beliefs about five attributes: (1) the identity of the condition, including its label (e.g., asthma) and associated symptoms (e.g., wheezing, shortness of breath, and dizziness); (2) the cause of the condition (e.g., heredity or exposure to dust mites); (3) its timeline or duration, which may be acute (short term), cyclical (it comes and goes over time), or chronic; (4) its consequences (e.g., asthma interferes with one’s ability to play sports); and (5) the potential for its control or cure (e.g., it can be controlled using inhalers and medication). This representation guides the selection of coping behaviors for controlling the health threat (e.g., seeking medical care or using an inhaler), and the outcomes are appraised in terms of their success in doing so (e.g., whether the wheezing has subsided). The representation and coping behaviors are then revised accordingly.
At the same time that the health threat cues activate the problem-focused self-regulation process, they trigger emotional responses such as fear and distress. The experience of wheezing and breathing difficulties can evoke feelings of panic, for example, and activation of representational beliefs about asthma can further enhance distress and worry. Awareness of these emotions (the emotional representation) motivates the use of actions to alleviate them (e.g., seeking support from a friend). The outcomes of these behaviors are then appraised for their success in reducing distress, and these appraisals feedback to revise the emotional representation and coping efforts.
Illness representations and emotional distress often motivate the same coping behaviors (e.g., use of an inhaler). At times, however, they can motivate conflicting actions. For example, fear arousal can lead to avoidance of disease detection behaviors even when the individuals’ beliefs motivate the use of these techniques. In a 1966 study of cigarette smokers conducted by Leventhal and Jean Watts, for example, those who viewed a fear-arousing program about lung cancer were less likely than those viewing an alternative program to agree to undergo a chest x-ray.
Empirical Evidence for the Commonsense Model
Numerous studies provide evidence that the five representational beliefs identified by the commonsense model predict a wide variety of illness behaviors and outcomes. In patients with chronic illnesses, beliefs of a chronic timeline and serious consequences tend to be associated with avoidance tendencies and poor psychological adjustment, whereas beliefs that an illness is controllable predict greater use of active, problem-focused coping strategies and greater psychological well-being. Research also demonstrates that emotional distress influences health-protective behaviors in ways that are predicted by the self-regulation model. For example, distress has been found to promote protective behaviors such as performing breast self-examinations and seeking medical care for unusual symptoms. However, distress may promote protective behavior only when an individual has a specific plan for engaging in that behavior. In one illustrative study conducted by Leventhal, Robert Singer, and Susan Jones in 1965, individuals who received fear-arousing messages about the dangers of tetanus reported strong intentions to get a tetanus shot, but only those who received assistance in developing action plans for obtaining the vaccinations were likely to do so in the subsequent weeks.
Conclusion
Self-regulation models provide frameworks for understanding goal-directed health behavior, whether the goals involve improving health or avoiding illness. Carver and Scheier’s model proposes that goals have a hierarchical organization, moving from more abstract goals down to more specific action goals. Emotions provide important feedback about one’s progress in achieving goals, and expectancies critically influence decisions to continue efforts or to give up. Dispositional optimism, a tendency to have positive outcome expectancies, has been found to be associated with favorable health outcomes. Leventhal’s commonsense model proposes that health threats activate both problem-focused and emotion-focused self-regulation. At the problem-focused level, behavior is guided by representational beliefs about the health threat’s identity, cause, timeline, consequences, and potential for control or cure. The use of self-regulation models to address behavioral health issues is yielding new insights into how cognitions, emotions, and feedback processes influence health-related behaviors and outcomes.
References:
- Baker, R. C, & Kirschenbaum, D. S. (1993). Self-monitoring may be necessary for successful weight control. Behavior Therapy, 24, 337-394.
- Brownlee, S., Leventhal, H., & Leventhal, E. A. (2000). Regulation, self-regulation, and construction of the self in the maintenance of physical health. In M. Boekarts, P. R. Pintrich, & M. Zeidner (Eds.), Handbook of self-regulation (pp. 369-416). San Diego, CA: Academic.
- Cameron, L. D., & Leventhal, H. (2003). The self-regulation of health and illness behaviour. London: Routledge.
- Carver, C. S., & Scheier, M. E (1998). On the self-regulation of behavior. New York: Cambridge University Press.
- Hagger, M. S., & Orbell, S. (2003). A meta-analytic review of the commonsense model of illness representations. Psychology and Health, 18, 141-184.
- Leventhal, H., Leventhal, E. A., & Cameron, L. D. (2001). Representations, proecedures, and affect in illness self-regulation: A perceptual—cognitive model. In A. Baum, T. Revenson, & J. E. Singer (eds.), Handbook of health psychology {pp. 19-47). Hillsdale, NJ: Erlbaum.
- Leventhal, H., Singer, R., & Jones, S. (1965). Effects of fear and specificity of recommendations upon attitudes and behavior. Journal of Personality and Social Psychology, 2, 20-29.
- Leventhal, H., & Watts, J. C. (1966). Sources of resistance to fear-arousing communications on smoking and lung cancer. Journal of Personality, 36, 154-168.
- Scheier, M. E, & Carver, C. S. (2003). Goals and confidence as self-regulatory elements underlying health and illness behavior. In L. D. Cameron & H. Leventhal (Eds.), The self-regulation of health and illness behaviour (pp. 17-41). London: Routledge.
- Scheier, M. E, Matthews, K. A., Owens, J. E, Magovern, G. J., Lefebvre, R. C, Abbott, R. A., & Carver, C. S. (1989). Dispositional optimism and recovery from coronary artery bypass surgery: The beneficial effects on physical and psychological well-being. Journal of Personality and Social Psychology, 57, 1024-1040.
- Scheier, M. E, Matthews, K. A., Owens, J. E, Schulz, R., Bridges, M. W, Magovern, G. J., Sr., & Carver, C. S. (1999). Optimism and rehospitalization following coronary artery bypass graft surgery. Archives of Internal Medicine, 159, 829-835.
Back to Health Psychology.