Stress management is the use of psychological interventions to reduce physical reactions (such as muscle tension, high blood pressure, insomnia, and gastric discomfort) to demanding environmental situations. These uncomfortable reactions may be associated with negative states such as anxiety, depression, anger, pain, or illness. Reduction of discomfort may be achieved by directly counteracting the stress through relaxation, by changing one’s view of the situation (reappraisal) or by changing the situation (e.g., increasing the use of available social support). In addition, where it is known that a stressful situation is forthcoming, such as surgery, advance training in stress management techniques (stress inoculation) may be very helpful. A combination of these techniques has been called the cognitive-behavioral approach to stress management. Stress management is the most fundamental psychological therapy in health psychology.
Relaxation, Meditation, and Attempts to Reduce Arousal
The use of relaxation to combat stress predates Hans Selye’s brilliant analysis defining stress in 1950. In 1929, Edmund Jacobson proposed progressive relaxation to deal with muscle tension. The Jacobson technique relies heavily on the assessment of muscle tension and the reduction of activity in the muscles. He concluded that muscle tension was important in the formation of high blood pressure, ulcers, and other diseases. Relaxation has been demonstrated to be helpful in limiting acute stress effects as well. For example, Janice Kiecolt-Glazer and her colleagues at Ohio University found positive effects of relaxation in regulation of the immune system affected by acute stress.
Harvard’s Herbert Benson noted that many cultures have developed meditative traditions that are very helpful in inducing muscle relaxation and other benefits. Benson observed that relaxation interventions in muscle tension have a long history dating back to antiquity.
Progressive relaxation, especially in an abbreviated 15- to 20-min form, has been a very popular technique in clinical practice. An individual tenses and relaxes each muscle group of the body progressively working from one area to the next and then concludes with general deep relaxation. Jacobson observed that perception of high muscle tension adapts so that one cannot feel tension after it is prolonged. The technique is a fairly active one. Muscles can relax more after tension or exercise than after not tensing. This may have something to do with the health benefits of exercise. For example, Kenneth Cooper and his colleagues in Texas found a significant relationship between death from all causes and low fitness. An additional benefit is that instructions for progressive relaxation can be tape recorded and one can achieve a degree of control over the time spent in relaxation. Variations on the progressive relaxation technique have been a cornerstone of stress management for decades.
A relaxation program may incorporate a variety of techniques to avoid boredom. A specific program may be tailored to the background of the individual. The Benson meditative technique promotes focusing on a slowly repeated sound image while in a comfortable position away from distractions. This is a very portable technique, which requires no equipment, and may be adapted to special conditions like walking for angina patients. Individuals with a religious orientation may gain the benefit of spirituality in repetitions of a certain sound or name. The mindfulness meditation promoted by Jon Kabat-Zinn has the advantage of concentrating on the “here and now” and is very consistent with some cognitive therapy approaches. The mental imagery approaches of Anees and Katherina Sheikh involve visualizing oneself in a safe, unstressed, desirable situation for a specified amount of time. This may logically appeal to people with high powers of imagination and offer a temporary distraction. The autogenic, or self-generated, relaxation described by Wolfgang Luthe is often incorporated into other approaches; for example, on a tape for progressive relaxation one might instruct a person to imagine their hands warming. Hypnosis (the use of suggestion) or biofeedback (the use of monitoring instrumentation) in assisting relaxation may be helpful, but individual differences in appeal and capability must be considered as well as expense. Breath control techniques have not been as useful as one might expect. Perhaps, as Stephen Porges and his colleagues at the University of Maryland found, some stress may be created in trying to control breathing. Whereas the techniques vary and the cognitive benefits may differ, the use of these techniques in stress management has the primary goal of reducing muscle tension and physiological arousal. Stanford’s Richard Lazarus and Susan Folkman would classify these approaches as emotion-focused coping because relaxation diminishes the arousal and the emotional state.
Reappraisal
Lazarus’s early research indicated that individual interpretation of situations is very important with respect to the nature of the stress effects. He observed a paradoxically high arousal in measures associated with emotional sweating in Japanese students watching a control film that did not seem to stress American students. His questions, after the experiment, led to the observation that the Japanese students were more upset at the possibility of having their emotions revealed by the instruments than were the Americans. Lazarus and Folkman took this cultural difference and other observations to suggest that stressed individuals could reappraise their situation to view it as not as stressful.
Researchers have observed that certain approaches to reappraisal may be effective. The perception of helplessness seems to be particularly stressful, and anything that can be done to make the individual feel less hopeless and more in charge is beneficial. As noted, Lazarus and Folkman offered an analysis of coping techniques based on a focus on the problem versus a focus on the emotion to assist the stressed individuals in understanding how to reappraise the situation. Susan Kobasa concluded that those hardy individuals who feel more in control, are more committed, and accept situations as a challenge are less likely to report stress effects than their counterparts. These cognitive attitudes can be taught in stress management programs. Significantly, Rod Martin of the University of Western Ontario in Canada concluded that the relationship between humor, health, and longevity has not been consistently found, and studies that support this relationship may have been flawed methodologically. Thus it seems appropriate to work on a reappraisal of the situation rather than on humor as a distraction. In Lazarus and Folkman’s terminology, this would be a problem-focused method of coping.
Changing the Stressor
The stressed individual often has much more control of the stressful situation than is perceived. Barbara and Irwin Sarason and many others have noted that individuals who perceive high social support do better with stressors. Sheldon Cohen and Leonard Syme’s anthology on social support and health also documents this relationship. Those with low social support may actually be under more stress than their counterparts, but these individuals may be counseled to increase social support by increasing contact with supportive relatives and friends and thus reduce the stress. People under stress can also seek to make new relationships in new environments through supportive counseling. Patients with the stress of a disease may excessively limit themselves socially and increase their stress due to loneliness. Education and counseling may reveal that limitations are not as severe as perceived. Support groups often serve this function. Vocational, financial, and interpersonal counseling may also be tools for effectively changing the environmental issues at hand. Therefore these interventions could also be described as problem focused.
Stress Inoculation
Donald Meichenbaum at the University of Waterloo in Canada has advocated the very logical concept of teaching management techniques before the stress as an inoculation against that stress. Stress effects include mental confusion and emotional responses that make it difficult for the stressed individual to effectively engage in appropriate interventions. Emmelkamp and his colleagues from the Netherlands concluded that short-term, after-the-fact, therapies like critical incident stress debriefing have not been as effective as hoped in reducing the risk of post-traumatic stress syndrome. These quick interventions do provide some immediate comfort and contacts for further therapy when that is necessary, but unfortunately do not apparently meet the primary goal of preventing serious stress reactions. The stress inoculation methods have been adapted to after-the-fact situations because stress tends to cycle with memories of the traumatic event. However, Foa and her colleagues at the University of Pennsylvania found that exposure therapy, in which a patient gradually confronts stressful situations, has longer-lasting benefits than stress inoculation after the trauma. When individuals are relatively unstressed before surgery or predictable emergencies, it would be very prudent for them to understand the stress management techniques of conceptualization, skills acquisition, and rehearsal and to have practiced the skills involved as Meichenbaum has suggested. Perhaps these beneficial skills should be a standard part of the education system.
Cognitive-Behavioral Modification
Cognitive—behavioral approaches integrate stress management techniques and offer increased benefit over single techniques. Many cognitive-behavioral approaches integrate behavioral with medical interventions in a multidisciplinary approach. For example, Kenneth Holroyd and fellow researchers at Ohio University concluded that cognitive techniques and medication can be combined to treat tension headaches. The physician Dean Ornish has created a lifestyle change program, which includes stress management, exercise, and dietary control to regulate cardiovascular disease. When one emotional reaction or pain is evident, cognitive-behavioral interventions may focus on that condition as in anger, anxiety, depression, and pain management. Cognitive-behavioral interventions show the best promise in management of stress, probably because of their eclectic nature.
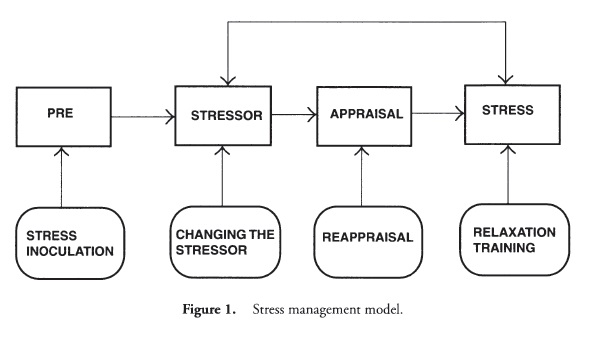
Stress management can involve interventions at every level of a stress model (Figure 1). These include the stress reaction (relaxation and exercise), the appraisal of the situation (reappraisal), the stressor itself (changing the situation), and even before the environmental demand (stress inoculation), A combination of techniques (cognitive-behavior modification) perhaps integrated with physical medicine (multidisciplinary approach) seems to offer advantages. Such techniques may focus on specific emotions or stresses as in anger, anxiety, depression, or pain management.
References:
- Alden, A., Dale, J. A., & DeGood, D. E. (2001). Interaction effects of affective state and focus of mental imagery on pain analgesia. Applied Psychophysiology and Biofeedback, 26, 117-126.
- Benson, H. (1975). The relaxation response. New York: Morrow.
- Blair, S. N., Kohl III, H. W., Paffenbarger, R. S., Clark, D. G., Cooper, K. H., & Gibbons, L. W. (1989). Physical fitness and all-cause mortality: A prospective study of men and women. Journal of the American Medical Association, 262, 2395-2402.
- Cohen, S., & Syme, S. L. (Eds.) (1985). Social support and health. Orlando, FLA: Academic.
- Coyne, J. C., & Racioppo, M. W. (2000). Never the twain shall meet? Closing the gap between coping research and clinical intervention research. American Psychologist, 55, 655-675.
- Dale, J. A., & DeGood, D. E. (1997-98). The emerging role of the psychologist in pain management. Advances in Medical Psychotherapy, 9, 1-20.
- DeGood, D. E. (1997). The headache and neck pain workbook. Oakland, CA: New Harbinger.
- DeGood, D. E., Crawford, A. L., & Jongsma, A. E., Jr. (1999). The behavioral medicine treatment planner. New York: Wiley.
- Foa, E. B., Dancu, C. V., Hembree, E. A., Jaycox, L. H., Meadows, E. A., & Street, G. P. (1999). A comparison of exposure therapy, stress inoculation training, and their combination for reducing posttraumatic stress disorder in female assault victims. Journal of Consulting and Clinical Psychology, 67, 194-211.
- Folkman, S., & Moskowitz, J. T. (2000). Positive affect and the other side of coping. American Psychologist, 55, 647—655.
- Hermann, C., Blanchard, E. B., & Flor, H. (1997). Biofeedback treatment for pediatric migraine: Prediction of treatment outcome. Journal of Consulting and Clinical Psychology, 65, 611-617.
- Holroyd, K. A., O’Donnell, E J., Stensland, M., Lipchik, G. L., Cordingley, G. E., & Carlson, B. W. (2001). Management of chronic tension-type headache with tricyclic antidepressant medication, stress management therapy, and their combination: A randomized controlled trial. Journal of the American Medical Association, 285, 2208-2220.
- Jacobson, E. (1929). Progressive relaxation: A physiological and clinical investigation of muscular states and their significance in psychology and medical practice. Chicago: University of Chicago Press.
- Kabat-Zinn, J. (1995). Wherever you go there you are: Mindfulness meditation in everyday life. New York: Hyperion.
- Kiecolt-Glaser, J. K., Marucha, P. T, Atkinson, C., & Glaser, R. (2001). Hypnosis as a modulator of cellular immune dysregulation during acute stress. Journal of Consulting and Clinical Psychology, 69, 674-682.
- Kobasa, S. C. (1979). Stressful life events, personality, and health: An inquiry into hardiness. Journal of Personality and Social Psychology, 37, 1-11.
- Lazarus, R. S. (1966). Psychobgical stress and the coping process. New York: McGraw-Hill.
- Lazarus, R., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer.
- Luthe, W. (1969). Dynamics of autogenic neutralization. New York: Grune & Stratton.
- Martin, R. (2001). Humor, laughter, and physical health: Methodological issues and research findings. Psychobgical Bulletin, 127, 504-519.
- Meichenbaum, D. (1977). Cognitive—behavior modification: An integrative approach. New York: Plenum.
- Meichenbaum, D. (1985). Stress inocubtion training. New York: Pergamon.
- Meichenbaum, D. (1996). Stress inoculation training for coping with stressors. Clinical Psychologist, 49, 4-7.
- Ornish, D., Scherwitz, L. W, Billings J. H., Gould, K. L., Merritt, T. A., Spader, S., et al. (1998). Intensive lifestyle changes for reversal of coronary heart disease. Journal of the American Medical Association, 280, 2001.
- Pierce, G. R., Sarason, B., & Sarason, I. (1992). General and specific support expectations and stress as predictors of perceived supportiveness: An experimental study. Journal of Personality and Social Psychology, 63, 297-307.
- Sargunaraj, D., Lehhrer, P., Hochron, S. M., Raush, L., Edelberg, Robert, P., & Stephen, W. (1996). Cardiac rhythm effects of ,125-hz paced breathing through a resistive load: Implications for paced breathing therapy and the polyvagal theory. Biofeedback and Self-Regubtion, 21, 131-147.
- Selye, H. (1950). The physiobgy and pathology of exposure to stress; a treatise based on the concepts of the general-adaptation-syndrome and the diseases of adaptation. Montreal: Acta.
- Selye, H. (1956). The stress of life. New York: McGraw-Hill.
- Seye, H. (Ed.). (1980). Selye’s guide to stress research. New York: Van Nostrand Reinhold.
- Sheikh, A., & Sheikh, K. (Eds.). (1989). Eastern and Western approaches to healing: Ancient wisdom and modern knowledge. New York: Wiley.
- Suinn, R. (2001). The terrible twos—anger and anxiety: Hazardous to your health. American Psychologist, 56, 27-32.
- van Emmerik, A. A. P., Kamphuis, J. H., Hulsbosch, A. M., & Emmelkamp, P. M. G. (2002). Single session debriefing after psychological trauma: A meta-analysis. Lancet, 360, 766-775.
Back to Health Psychology.