Neuropsychology Definition and Historical Background
The field of neuropsychology is concerned with the relationship between the brain and behavior. “Behavior” in this definition refers not only to observable actions, but also to internal cognitive processes such as memory, attention, visual functions, decision making, and emotions. The term neuropsychology is most often applied to the study of the relationship between brain and behavior in humans, although clearly it could also be applied to the study of animals. In health psychology, the term clinical neuropsychologist is used to denote a psychologist with expertise in how brain-behavior relationships are relevant to the diagnosis, treatment, and well-being of patients with known or suspected brain disease.
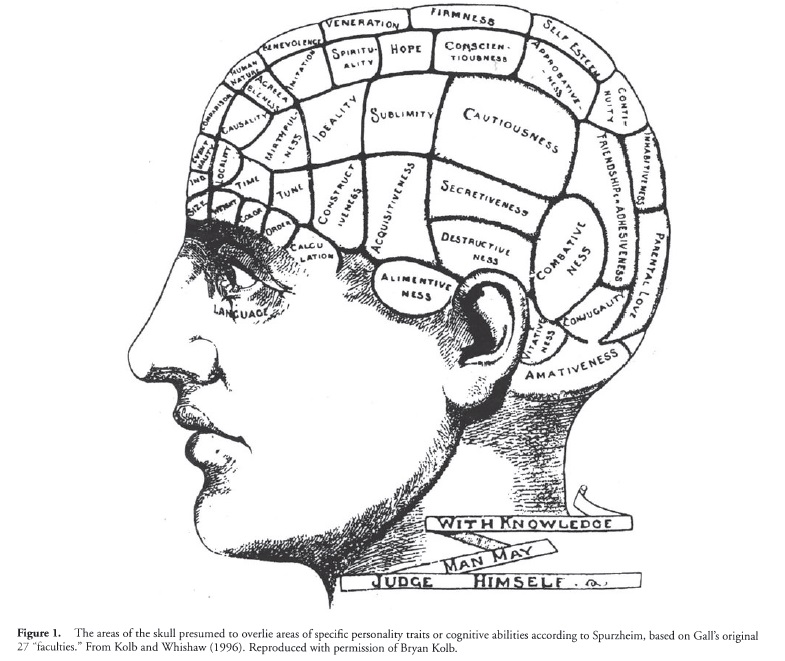
The history of neuropsychology in some senses dates back to the early Greeks. However, the beginning of the modern age is most often linked to the 19th century. In the early 1800s Franz Josef Gall (1758-1828) and Johann Casper Spurzheim (17761832) proposed that different areas of the brain are dedicated to different traits or abilities and that differences in the shape of the skull would reflect the strength or weakness of underlying “faculties” (see Figure 1). This localizationist approach, called phrenology, was influential in England and the United States. It was not long after this that Paul Broca (1824-1880) reported a relationship between language impairments and damage to the left frontal lobe, and Carl Wernicke (1848-1904) subsequently described a different set of language impairments associated with a different part of the left hemisphere. What followed was a series of discoveries by late 19th-century neurologists and psychiatrists concerning some of the fundamental relationships between different areas of the brain and specific behaviors [see Benton (1988) for a review].
By the mid-20th century, psychologists were beginning to investigate how specific tests were performed by patients with brain damage. It was around this time that the term neuropsychology was coined. Early pioneers in this area include Ward Halstead, Arthur Benton, Ralph Reitan, Brenda Milner, and Edith Kaplan. Neuropsychological batteries, or specific collections of mental tests that proved sensitive to brain damage, were developed by the 1940s and 1950s. Other early neuropsychologists developed formal tests of language, memory, attention, and other cognitive capacities that proved sensitive not only to brain damage generally, but also to specific areas of brain damage.
The advent of neuroimaging techniques such as computerized tomography (CT) in the 1970s and magnetic resonance imaging (MRI) in the 1980s marked the beginning of the most recent major advances in neuropsychology. Until that time, researchers often had to wait until autopsy of the brain to establish a relationship between areas of brain damage and neuropsychological impairment. However, neuroimaging techniques allowed neuropsychologists to examine, in living humans, the relationship between specific areas of brain damage and performance on standardized mental tests. This resulted in an explosion of knowledge in relation to brain function, culminating in the “decade of the brain” of the 1990s. Alongside these neuroimaging techniques, which enable researchers to see the brain in living humans, are newer “functional” neuroimaging techniques such as functional MRI (fMRI) and positron emission tomography (PET), which allow researchers to evaluate areas of the brain that are utilized during different mental tasks.
Training in Neuropsychology
Clinical neuropsychology is a practice-oriented subspecialty of clinical psychology that aims to evaluate or treat behavioral deficits produced by brain damage or dysfunction. Clear guidelines for training have been published (Hannay et al., 1998). Training usually begins with an undergraduate degree in psychology. After they obtain a college degree, students typically enroll in a graduate program in clinical psychology that is approved by the American Psychological Association or other appropriate national organization. The end point of such a graduate program is the doctoral (PhD) degree. Attainment of the doctoral degree requires both breadth and depth in the field of psychology, including study in areas such as statistics and methodology, social psychology, and biological bases of behavior, in addition to more clinically oriented areas of training such as psychopathology, interviewing and assessment techniques, and professional ethics. During graduate training, students who want to become clinical neuropsychologists generally also study areas more specific to that specialty, including functional and structural neuroanatomy, neurological and medical disorders related to behavioral or cognitive change, psychopharmacology, and entry-level classes in the practice of neuropsychology. Graduate training usually takes 5—6 years and includes 1 year of full-time supervised clinical internship prior to the granting of the PhD degree. The clinical internship usually includes at least one major rotation in neuropsychology for those students wanting to specialize in the field.
The last stage of training in clinical neuropsychology is the residency. After they obtain the PhD degree, students of neuropsychology complete a 2-year residency aimed at further training in the specialty of clinical neuropsychology. It is at this level that students branch out in the specialty area, principally through supervised training in specific neuropsychological procedures. These specific procedures include all aspects of assessment including knowledge of measures and tests, report writing, and detailed knowledge of medical, psychiatric, and neurological conditions in relation to behavior and cognition change. In recent years, additional training in neuropsychological rehabilitation has been offered with increasing frequency. The residency is a 2-year program, and is viewed as a mandatory part of training in clinical neuropsychology. Research is viewed as a fundamental component of this stage, and most residency programs in clinical neuropsychology provide time for independent and collaborative research. The residency is generally considered to be complete after 2 years, assuming the resident shows evidence of competence in all relevant areas. Board certification can be obtained following residency training through the American Board of Clinical Neuropsychology (ABCN), which is affiliated with the American Board of Professional Psychology (ABPP). The ABCN-ABPP serves to designate individuals who have undergone extensive written and practice examinations of their competence as clinical neuropsychologists.
Activities of a Neuropsychologist
Clinical
Most neuropsychologists maintain a clinical practice. In a clinical setting, neuropsychologists typically administer and interpret the results of standardized tests of mental and behavioral ability. There can be many reasons for such an assessment. For example, the results of neuropsychological assessments may be used to determine the management of patients with brain disease, such as a person’s ability to handle finances, drive, or live independently. Also, such assessments are often used to monitor the recovery of cognitive abilities following certain brain disorders (e.g., stroke) or the rate and nature of cognitive decline in progressive conditions (e.g., Alzheimer’s disease). Finally, in some disorders (e.g., mild traumatic brain injury) all other medical tests may be normal and neuropsychological assessment may be the only means by which to establish the diagnosis.
There are many methods and several schools of assessment, but all have in common the fact that tests are standardized and based on published scientific normative data. A neuropsychological assessment typically takes from 2 to 6 hr of patient time, depending on the referral question, the stamina of the patient, and the results of other tests. Screening examinations may last as little as 30 min, and extended examinations may last 8 hr or more. It is common to measure multiple cognitive abilities in the course of a single assessment, including memory and orientation, language, higher visual functions, spatial abilities, decision-making ability, and mood and personality.
Research
Many neuropsychologists conduct research, particularly in academic settings such as university departments of psychology or in medical schools. Usually, the aim of such research is to examine the relationship between the brain and behavior. For example, many neuropsychologists study the relationship between the structure of the brain and a person’s ability to produce language, have memory, or have normal vision. Although such studies can be traced to discoveries from the mid-19th century, it is fair to say that most modern knowledge of the relationship between the brain and behavior has been derived from research in the last 30-50 years. Such research has yielded information now considered to be fundamental in the diagnosis of many disorders. For example, neuropsychological research has substantiated the fact that early memory impairments are the hallmark of Alzheimer’s disease, which in turn has helped with early diagnosis of the condition. This early diagnosis of Alzheimer’s disease has helped clinicians to provide more timely interventions for patients with the disorder, and has thereby improved the quality of life for millions of patients.
More recent neuropsychological research has focused on treatment and rehabilitation of acquired brain problems such as memory disorders (amnesia), language disorders, and vision impairments. For example, recent studies have begun to investigate ways in which patients with amnesia following stroke may benefit most from memory aids, using tools such as notebooks, pagers, handheld computers, and other automatic reminders and mnemonic strategies. This research is in its infancy, but reflects a straightforward application of neuropsychological principles developed in the last 50 years to the direct alleviation of suffering due to acquired cognitive impairments.
Teaching
Many neuropsychologists are in academic settings, and in that context those neuropsychologists typically have responsibilities that include teaching at the college level or in graduate schools or medical schools. Neuropsychologists, given that they are usually trained as clinical psychologists, often have basic teaching responsibilities in departments of psychology. Courses taught might include introductory courses in psychology and clinical psychology, but typically also include advanced courses in assessment, brain function, clinical neuropsychological assessment, and psychopharmacology. Similarly, neuropsychologists employed in medical schools often teach medical students or medical residents about the fundamentals of clinical neuropsychology and brain-behavior relationships. Particularly in departments of neurology and psychiatry, it is a common part of a young physician’s training to learn about formal neuropsychological assessment and the ways that such assessment may benefit patients.
References:
- Benton, A. L. (1988) Neuropsychology: Past, present, and future. In F. Boiler &c J. Grafman (Eds.), Handbook of neuropsychology (Vol. 1, pp. 00-00). Amsterdam: Elsevier Science.
- Hannay, H. J., Bieliauskas, L. A., Crosson, B. A., Hammeke, T. A., Hamsher, K. deS., & Coffer, S. P. (1998). Proceedings: The Houston conference on specialty education and training in clinical neuropsychology. Archives of Clinical Neuropsychology, 13, 157-249.
- Kolb, B., & Whishaw, I. Q. (1996). Fundamental of human neuropsychology (4th ed.). New York: Freeman.
Back to Health Psychology.